 viruspox.com
viruspox.com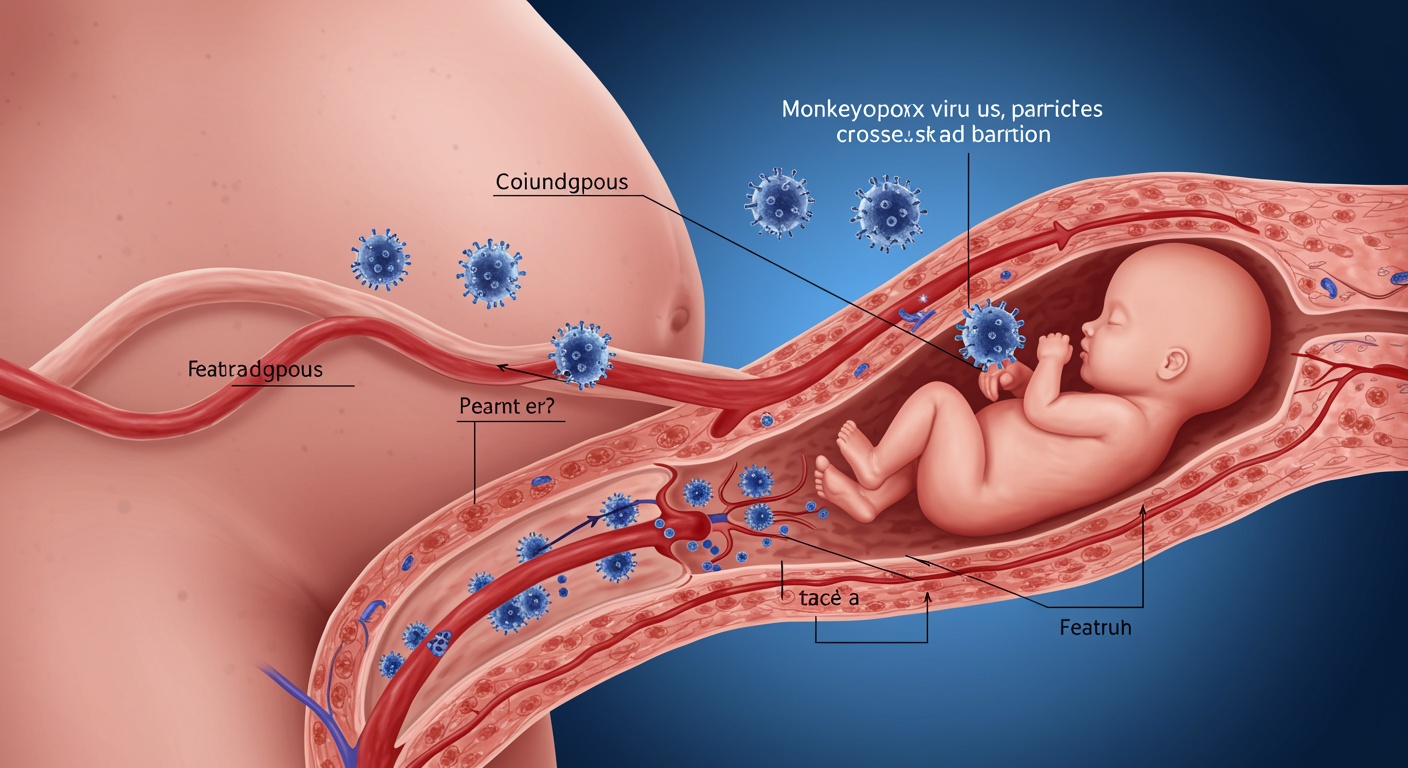
The resurgence of mpox (formerly monkeypox) as a global health concern has brought unprecedented attention to its impact on vulnerable populations, particularly pregnant women and children. While historically considered a rare zoonotic disease confined to Central and West Africa, the emergence of human-to-human transmission patterns has fundamentally altered our understanding of mpox epidemiology and necessitated urgent evaluation of its effects on maternal-fetal health. The orthopoxvirus genus, to which the monkeypox virus belongs, has a well-documented history of causing severe complications during pregnancy, as evidenced by historical smallpox data. This comprehensive analysis examines the current evidence regarding mpox infection during pregnancy and in pediatric populations, with particular emphasis on vertical transmission mechanisms, clinical presentations, and maternal-fetal outcomes.
The significance of understanding mpox in pregnancy extends beyond individual patient care to encompass broader public health implications. Pregnant women represent a uniquely vulnerable population due to physiological immunosuppression that facilitates fetal tolerance while potentially increasing susceptibility to viral infections. The developing fetus faces additional risks through potential vertical transmission, which can occur via transplacental, intrapartum, or postnatal routes. Current evidence suggests that mpox shares many characteristics with its closely related orthopoxvirus cousin, variola virus, particularly regarding its propensity for vertical transmission and adverse pregnancy outcomes.
Pathophysiology and Transmission Mechanisms
Understanding the pathophysiology of mpox infection during pregnancy requires examination of both maternal immune responses and potential routes of vertical transmission. The monkeypox virus demonstrates remarkable similarity to variola virus in its cellular tropism and replication patterns, suggesting comparable mechanisms of maternal-fetal transmission. Following initial infection, the virus undergoes primary replication at the inoculation site before disseminating through lymphatic channels to regional lymph nodes. This process triggers primary viremia, during which the virus can potentially cross the placental barrier and establish fetal infection.
The placental barrier, while effective against many pathogens, demonstrates variable permeability to different orthopoxviruses. Historical studies of smallpox during pregnancy revealed that variola virus could readily traverse the placental interface, leading to high rates of fetal infection and mortality. Emerging evidence suggests that monkeypox virus possesses similar transplacental transmission capabilities, with viral loads detected in fetal tissues and placental specimens reaching concentrations exceeding one million copies per milliliter. This high viral burden correlates strongly with adverse pregnancy outcomes, including spontaneous abortion, stillbirth, and congenital infection.
The immunological changes inherent to pregnancy may exacerbate mpox infection severity and duration. Pregnancy-associated immunosuppression, characterized by shifts in T-helper cell populations and altered cytokine profiles, can impair the maternal immune response to viral infections. This immunological alteration serves the evolutionary purpose of preventing fetal rejection but simultaneously increases maternal susceptibility to infectious diseases. The combination of heightened viral replication potential and diminished immune clearance creates conditions favorable for sustained viremia and increased likelihood of vertical transmission.
Clinical Manifestations in Pregnancy
Mpox infection during pregnancy presents with clinical features that may differ significantly from those observed in non-pregnant adults. The characteristic biphasic illness pattern, consisting of a prodromal phase followed by rash development, remains consistent but may be modified by pregnancy-related physiological changes. The prodromal phase typically includes fever, headache, myalgia, and lymphadenopathy, symptoms that may be initially attributed to common pregnancy-related complaints or other infectious processes.
The progression from prodromal symptoms to cutaneous manifestations follows a predictable timeline, with rash development occurring approximately two to four days after fever onset. The rash evolution through macular, papular, vesicular, and pustular stages mirrors that seen in non-pregnant individuals, but the overall disease course may be more severe and prolonged. Pregnant women appear to experience higher rates of secondary bacterial infections, prolonged viral shedding, and increased risk of complications such as pneumonia and encephalitis.
Maternal mortality rates associated with mpox infection during pregnancy vary significantly based on viral clade and gestational timing. Historical data from Central Africa suggest case fatality rates approaching ten percent for clade I infections, while more recent data from clade II outbreaks indicate lower but still significant mortality risks. The physiological stress imposed by severe mpox infection can precipitate obstetric complications including preterm labor, placental abruption, and hemorrhage, further contributing to maternal morbidity and mortality.
Vertical Transmission and Fetal Outcomes
The capacity for vertical transmission represents one of the most concerning aspects of mpox infection during pregnancy. Multiple transmission routes have been documented, including transplacental passage during pregnancy, intrapartum exposure during delivery, and postnatal transmission through close contact or potentially through breastfeeding. The efficiency of each transmission route varies based on gestational timing, maternal viral load, and duration of exposure.
Transplacental transmission appears most likely during periods of peak maternal viremia, typically occurring during the first week of symptomatic illness. The developing placental vasculature and immature fetal immune system provide minimal barriers to viral invasion, particularly during early pregnancy when organogenesis is occurring. Fetal infection during the first trimester carries the highest risk of embryonic death and spontaneous abortion, while second and third-trimester infections may result in stillbirth, premature delivery, or congenital disease.
Recent case reports have documented vertical transmission of clade Ib mpox virus, providing molecular evidence of maternal-fetal transmission across all pregnancy trimesters. These cases demonstrated varying outcomes ranging from early pregnancy loss to successful delivery of infected infants. The variability in outcomes likely reflects differences in gestational timing at infection, maternal immune status, viral load, and access to supportive care. Notably, some cases involved detection of viral DNA in fetal tissues at concentrations exceeding those found in maternal blood, suggesting active fetal replication rather than passive transfer.
Pediatric Mpox Considerations
Children represent another vulnerable population with distinct susceptibility patterns and clinical presentations. Pediatric mpox infections occur through various routes including vertical transmission from infected mothers, household contact exposure, and community transmission. The clinical course in children often mirrors that seen in adults but may be complicated by higher rates of severe disease, secondary bacterial infections, and systemic complications.
Neonates born to mothers with active mpox infection face particular risks due to immature immune systems and potential exposure through multiple routes. Intrauterine infection can result in congenital mpox syndrome, characterized by widespread cutaneous lesions, systemic organ involvement, and high mortality rates. Intrapartum transmission may occur through exposure to maternal lesions or infected birth canal secretions, while postnatal transmission can result from close contact during caregiving activities.
The differential diagnosis of mpox in pediatric populations requires careful consideration of other vesicular rash diseases including varicella, herpes simplex virus infection, and hand-foot-and-mouth disease. The characteristic centrifugal distribution of mpox lesions, presence of lymphadenopathy, and epidemiological risk factors help distinguish mpox from other conditions. However, atypical presentations may occur, particularly in very young children or those with underlying immunodeficiencies.
Diagnostic Considerations
Accurate and timely diagnosis of mpox during pregnancy requires a high index of suspicion combined with appropriate laboratory testing. The clinical presentation may be modified by pregnancy-related changes, necessitating careful evaluation of suspicious symptoms and potential exposures. Standard diagnostic approaches utilize polymerase chain reaction amplification of viral DNA from lesion specimens, which provides rapid and accurate identification of monkeypox virus with high sensitivity and specificity.
Specimen collection during pregnancy requires particular attention to patient comfort and safety while ensuring adequate sample quality for testing. Vesicular fluid, scab material, and lesion swabs represent optimal specimens for PCR testing, while blood samples may be useful during periods of active viremia. The timing of specimen collection relative to symptom onset affects test sensitivity, with highest yields obtained from fresh vesicular lesions during the first week of rash appearance.
Serological testing plays a limited role in acute diagnosis but may be useful for retrospective confirmation or epidemiological investigations. The presence of cross-reactive antibodies from previous smallpox vaccination or other orthopoxvirus exposures can complicate serological interpretation. Additionally, pregnancy-related immunological changes may affect antibody production and persistence, further limiting the utility of serological methods for acute diagnosis.
Management and Treatment Strategies
The management of mpox infection during pregnancy requires a multidisciplinary approach involving infectious disease specialists, obstetricians, pediatricians, and public health authorities. Treatment decisions must balance maternal health considerations with potential fetal risks, while implementing appropriate infection control measures to prevent healthcare-associated transmission. The limited availability of specific antiviral therapies necessitates careful consideration of risk-benefit ratios for each therapeutic intervention.
Tecovirimat represents the primary antiviral option for severe mpox infections, with approval for smallpox treatment and expanded access protocols for mpox under investigational new drug provisions. Animal studies have demonstrated no evidence of teratogenic effects at doses significantly exceeding recommended human dosing, providing reassurance regarding fetal safety. However, limited human pregnancy data necessitates careful consideration of treatment indications and close monitoring for adverse effects.
Supportive care measures form the cornerstone of mpox management during pregnancy, focusing on symptom relief, prevention of secondary complications, and maintenance of maternal-fetal well-being. Adequate hydration, pain management, and wound care help minimize discomfort and reduce infection risks. Close obstetric monitoring allows early detection of pregnancy complications including preterm labor, fetal distress, and placental abnormalities that may require intervention.
Isolation precautions during pregnancy require special consideration to balance infection control needs with maternal psychological well-being and family dynamics. Standard contact and droplet precautions are recommended for hospitalized patients, while home isolation may be appropriate for stable patients with adequate support systems. The duration of isolation should be based on clinical resolution of lesions and cessation of viral shedding rather than arbitrary time periods.
Prevention and Vaccination Strategies
Prevention of mpox infection during pregnancy relies primarily on risk reduction strategies and appropriate vaccination of susceptible individuals. The Modified Vaccinia Ankara vaccine demonstrates safety and efficacy for mpox prevention and is approved for use in pregnant women based on favorable safety profiles in animal studies and clinical experience with smallpox vaccination programs. Pre-exposure vaccination of women of reproductive age provides optimal protection, as post-exposure vaccination efficacy may be limited once infection is established.
Risk assessment and counseling for pregnant women should address potential exposure scenarios including travel to endemic areas, contact with suspected cases, and occupational exposures in healthcare settings. High-risk individuals may benefit from enhanced surveillance and early intervention strategies to minimize disease severity and transmission risks. Community education programs can help pregnant women recognize early symptoms and seek appropriate medical evaluation when indicated.
The timing of vaccination relative to pregnancy requires careful consideration of individual risk factors and vaccine availability. Pre-conception vaccination provides optimal protection without concerns about fetal exposure, while vaccination during pregnancy may be indicated for high-risk exposures or outbreak scenarios. Post-partum vaccination can provide protection for future pregnancies while potentially reducing transmission risks to newborn infants through passive antibody transfer.
Breastfeeding Considerations
The safety of breastfeeding during maternal mpox infection remains incompletely understood, with limited data available to guide clinical decision-making. Theoretical concerns include potential viral transmission through breast milk, close contact during feeding, and exposure to maternal lesions in the breast or nipple area. However, the absence of detectable viral DNA in breast milk samples from infected mothers suggests that milk itself may not represent a significant transmission route.
The decision regarding breastfeeding should be individualized based on maternal disease severity, presence of breast lesions, availability of safe alternatives, and family preferences. When breastfeeding is continued, strict precautions including careful hand hygiene, covering of lesions, and use of appropriate personal protective equipment may help reduce transmission risks. Expression and safe storage of breast milk may allow continued provision of maternal milk while minimizing direct contact exposure.
The immunological benefits of breastfeeding, including passive antibody transfer and enhanced infant immune development, must be weighed against potential transmission risks. In resource-limited settings where safe alternatives to breastfeeding may not be readily available, the balance may favor continued breastfeeding with appropriate precautions. Ongoing monitoring of both mother and infant allows early detection of transmission and prompt intervention if needed.
Long-term Outcomes and Follow-up
The long-term consequences of mpox infection during pregnancy remain incompletely characterized due to limited follow-up data and the relatively recent emergence of widespread human-to-human transmission. Available evidence suggests that surviving infants may experience developmental delays, immunological dysfunction, and increased susceptibility to secondary infections. However, the magnitude and persistence of these effects require further investigation through systematic longitudinal studies.
Maternal recovery following mpox infection during pregnancy generally follows patterns similar to those observed in non-pregnant adults, with complete resolution of cutaneous lesions and return to baseline functional status in most cases. However, some women may experience prolonged fatigue, mood disturbances, and cosmetic concerns related to scarring. Psychological support and counseling may be beneficial for women experiencing anxiety or depression related to their infection and concerns about fetal outcomes.
Future pregnancy planning for women with a history of mpox infection should include counseling regarding recurrence risks, which are generally considered low based on the development of long-lasting immunity following recovery. However, the possibility of reinfection with different viral clades or in the setting of severe immunosuppression cannot be entirely excluded. Preconception counseling and optimization of maternal health status may help ensure optimal outcomes in subsequent pregnancies.
Public Health Implications
The emergence of mpox as a global health threat with demonstrated capacity for vertical transmission carries significant public health implications requiring coordinated international response efforts. Surveillance systems must be adapted to capture pregnancy-associated cases and outcomes, enabling better understanding of disease patterns and risk factors. Enhanced reporting requirements for pregnant women with suspected or confirmed mpox infection can facilitate rapid investigation and implementation of control measures.
Healthcare system preparedness for mpox in pregnancy requires establishment of clinical protocols, training programs, and supply chain management for necessary medications and protective equipment. Specialized obstetric units may need enhanced isolation capabilities and staff training to manage infected pregnant women safely. Coordination between obstetric, pediatric, and infectious disease services ensures comprehensive care while maintaining appropriate infection control standards.
Contact tracing and outbreak investigation activities must account for the unique vulnerabilities of pregnant women and children, implementing targeted interventions to protect these high-risk populations. Close contacts who are pregnant or planning pregnancy may require enhanced monitoring, post-exposure prophylaxis, or vaccination depending on individual risk assessments. Community education campaigns should specifically address pregnancy-related concerns and provide clear guidance for risk reduction strategies.
Research Priorities and Future Directions
The limited evidence base regarding mpox in pregnancy and children highlights urgent research needs that must be addressed to inform evidence-based clinical practice and public health policy. Prospective cohort studies of pregnant women with mpox infection are needed to characterize clinical outcomes, transmission rates, and long-term consequences for both mothers and children. These studies should include diverse populations to account for potential differences in disease severity and outcomes based on genetic, nutritional, and socioeconomic factors.
Mechanistic studies investigating the pathophysiology of vertical transmission can provide insights into prevention strategies and treatment targets. Understanding the timing and efficiency of transplacental transmission, the role of maternal immune responses in protecting or facilitating fetal infection, and the impact of antiviral treatments on transmission risk will inform clinical management decisions. Additionally, investigation of viral factors that influence transmission efficiency may guide vaccine development and therapeutic interventions.
Clinical trials evaluating the safety and efficacy of antiviral treatments during pregnancy are essential for establishing evidence-based therapeutic protocols. These studies must carefully balance the ethical considerations of research in pregnant women with the urgent need for data to guide clinical practice. Collaborative international research networks can facilitate enrollment of adequate sample sizes while ensuring diverse representation across different populations and healthcare settings.
Conclusion
Mpox infection during pregnancy and in children represents a complex clinical challenge requiring multidisciplinary expertise and evidence-based management strategies. The demonstrated capacity for vertical transmission and potential for severe maternal and fetal outcomes necessitate heightened awareness among healthcare providers and implementation of comprehensive prevention and treatment protocols. While current evidence provides important insights into disease patterns and management approaches, significant knowledge gaps remain that require urgent research attention.
The global emergence of mpox transmission patterns that include vulnerable populations such as pregnant women and children underscores the importance of robust surveillance systems, healthcare system preparedness, and international cooperation in outbreak response efforts. As our understanding of this disease continues to evolve, clinical practice guidelines and public health policies must be regularly updated to reflect new evidence and changing epidemiological patterns.
Healthcare providers caring for pregnant women and children must maintain vigilance for mpox infection while implementing appropriate diagnostic and management strategies based on current evidence. The balance between maternal health, fetal well-being, and infection control requires careful consideration of individual risk factors and available interventions. Continued research efforts will undoubtedly refine our understanding of mpox in these vulnerable populations and improve outcomes for affected individuals and their families.
Table 1: Reported Pregnancy Outcomes in Mpox Infection
| Gestational Period | Outcome | Frequency (%) | Viral Clade | References |
| First Trimester | Spontaneous Abortion | 85-95 | I, II | Multiple case series |
| Second Trimester | Stillbirth | 45-60 | I, II | Limited case reports |
| Third Trimester | Preterm Delivery | 30-40 | II | Recent outbreak data |
| All Trimesters | Maternal Death | 15-34 | I | Historical data |
| All Trimesters | Live Birth | 40-55 | II | Contemporary reports |
Table 2: Clinical Features of Congenital Mpox Syndrome
| Clinical Feature | Frequency | Description | Severity |
| Cutaneous Lesions | >95% | Generalized vesiculopustular rash | Severe |
| Hepatomegaly | 70-80% | Enlarged liver with elevated enzymes | Moderate to Severe |
| Respiratory Distress | 60-70% | Pneumonia, respiratory failure | Severe |
| Neurological Involvement | 40-50% | Encephalitis, seizures | Severe |
| Growth Restriction | 80-90% | Low birth weight, stunting | Moderate |
| Mortality | 75-85% | Death within first month | Fatal |
Table 3: Risk Factors for Vertical Transmission
| Risk Factor | Relative Risk | Mechanism | Prevention Strategy |
| First Trimester Infection | 5.2 | Organogenesis vulnerability | Pre-conception vaccination |
| High Maternal Viral Load | 3.8 | Increased transplacental passage | Early antiviral treatment |
| Prolonged Illness | 2.9 | Extended exposure period | Supportive care optimization |
| Immunosuppression | 4.1 | Impaired viral clearance | Immune status assessment |
| Clade I Infection | 6.7 | Higher virulence | Enhanced surveillance |

